
Page 23 - 66 thorax49-55_opt
P. 23
CHAPTER 53
Chest Wall Deformities
Michael Singh
Dakshesh Parikh
Brian Kenney
Pectus Carinatum
Introduction
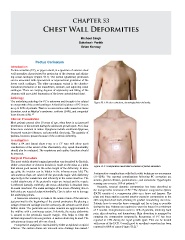
Pectus carinatum (PC), or pigeon chest, is a spectrum of anterior chest
wall anomalies characterised by protrusion of the sternum and adjoin-
ing costal cartilages (Figure 53.1). The sternal (gladiolus) protrusion
can be associated with symmetrical or asymmetrical protrusion of the
lower costal cartilages. The other uncommon variant is the chondro-
manubrial protrusion of the manubrium, sternum, and adjoining costal
cartilages. There are varying degrees of asymmetry and tilting of the
sternum with associated depression of the lower anteriolateral chest.
Aetiology
The underlying aetiology for PC is unknown and thought to be related
Figure 53.1: Pectus carinatum, chondrogladiolar deformity.
to overgrowth of the costal cartilages. A familial incidence of PC is seen
in up to 26% of patients. There is an association with connective tissue
disorders, such as Marfan’s syndrome, scoliosis (34%), and congenital
heart disease (6%). 1,2
Clinical Presentation
Most patients present after 10 years of age, when there is an increased
prominence of the sternum during the adolescent growth spurt. PC is four
times more common in males. Symptoms include exertional dyspnoea,
decreased exercise tolerance, and precordial chest pain. The majority of
patients, however, present because of the cosmetic deformity.
Investigation
Either a PA and lateral chest x-ray or a CT scan will allow good
visualisation of the extent of the abnormality. Any spinal abnormality
should also be evaluated. The respiratory and cardiac functions should
be assessed.
Surgical Procedure
The most widely adopted surgical procedure was described by Ravitch.
Either a transverse or chevron incision is made on the chest at a point Figure 53.2: Postoperative result after correction of pectus carinatum.
that allows good access to the entire length of the deformity. In teen-
age girls, the incision can be hidden in the inframammary fold. The
subcutaneous flaps are raised off the pectoralis major with diathermy Postoperative complications with the Ravitch technique are uncommon
superiorly to the manubrium and inferiorly to the rectus insertion. The (11–22%). The reported complications following PC correction are
medial attachments of the pectoralis major are incised and the muscle seroma, pleural effusion, pneumothorax, and atelectasis. Hypertrophic
1,2
is reflected laterally. Inferiorly, the rectus abdominis is detached from scarring can occur in 15% of patients.
its costal insertions. The costal cartilages of the lower offending ribs on Recently, external dynamic compression has been described as
2
both sides are resected subperichondrally. Care is taken not to damage the nonoperative treatment of PC. The dynamic compression system
the underlying pleura. (DCS) consists of a compression plate on a brace and harness. The
A transverse osteotomy is made in the anterior table of the sternum plate and brace applies external anterior posterior compression to the
just proximal to the beginning of the sternal protrusion. By placing a still compliant chest wall, allowing its gradual remodelling over time.
wedge of resected cartilage into the osteotomy, the sternum can be tilted Patients have to wear the brace overnight and for as long as possible
farther down. The pectoralis and rectus muscles are approximated in during the day. Patients are required to wear the brace for a minimum
the midline with a continuous suture. Inferiorly, the rectus abdominis of 7 months. Complications occur in 12% of patients, involving back
is sutured to the pectoralis muscle margin. This helps to keep the pain, skin ulceration, and haematoma. Skin ulceration is managed by
sternum depressed in its new position. A suction drain may be used. The stopping the compression temporarily. Recurrence of PC has been
subcutaneous tissues and skin are closed. reported in 15% during the rapid growth spurt. This can be treated
Postoperative analgesia is maintained by either an epidural or opioid with reuse of the DCS. Overall good to excellent correction has been
2
infusion. The suction drains are removed once drainage has ceased. reported in 88% of cases (Figure 53.2).
1