
Page 10 - 66 thorax49-55_opt
P. 10
CHAPTER 50
Achalasia
George G. Youngson
Lohfa B. Chirdan
Introduction Physical Examination
Achalasia is an uncommon oesophageal problem in children and conse- Similarly, physical examination covers a range of findings from mild
quently can be slow to diagnose. It is a condition of unknown aetiology weight loss to an advanced pulmonary sepsis and severe malnutri-
characterised by poor or absent motility of the body of the oesophagus tion. Achalasia can be associated with adrenocorticotropic hormone
and the failure of the lower oesophageal sphincter to relax. Infants may (ACTH)-resistant adrenal insufficiency and alacrima (an absence of
4
present with failure to thrive, pulmonary symptoms, vomiting, dyspha- tears). Hence, presentation may have the features of achalasia, addi-
gia, and growth retardation, but due to the rarity of the condition, many sonianism, and alacrima (triple A, or Allgrove syndrome). All other
children present late with any of the above symptoms as well as with physical findings are nonspecific.
significant nutritional compromise. In the absence of an identifiable Investigations
cause, treatment is directed at symptoms.
Chest x-ray can demonstrate an air-fluid level in the oesophagus with a
Demographics characteristic absence of the gastric air bubble on an erect film. In the
The prevalence of this condition is unclear; a worldwide survey of absence of standard facilities (as is the case in most centres in Africa
paediatric surgeons with experience in achalasia in childhood, how- and other developing countries), a high index of suspicion as well as
1
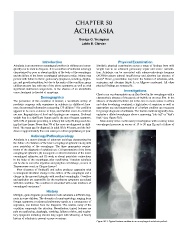
ever, documented information concerning 175 children. The condition appropriate use and interpretation of a barium swallow are necessary
appears to be more common in boys, and familial cases do exist but for prompt diagnosis of achalasia. The barium swallow typically dem-
are rare. Regurgitation of food and dysphagia are common. Profound onstrates a dilated oesophagus above a narrowing “rats tail” or “bird’s
weight loss is a significant feature and is the most frequent symptom, beak” (see Figure 50.1).
with 18% of patients presenting in infancy but only 6% diagnosed dur- Manometry is the confirmatory investigation with a resting lower
ing that time frame. Fewer than 5% of the cases are diagnosed in child- oesophageal pressure in excess of 15 to 20 mm Hg and a failure of
hood. The mean age for diagnosis in adult life is 45 years, and the inci-
dence is approximately five new cases per million population per year.
Aetiology/Pathophysiology
Achalasia is a motor disorder of unknown aetiology characterised by
the failure of relaxation of the lower oesophageal sphincter along with
poor peristalsis of the oesophagus. The three manometric require-
ments of the diagnosis of achalasia are: (1) hypertension of the lower
oesophageal sphincter, (2) incomplete or absent relaxation of the lower
oesophageal sphincter, and (3) weak or absent peristalsic contractions
in the body of the oesophagus after swallowing. Transient achalasia
can be due to corrosive ingestion and ganglion cell damage, as seen in
Trypanosoma cruzi, or Chagas disease. 2
Poor clearance of foodstuffs and saliva produces stagnation with
a consequent structural change in the calibre of the oesophagus and a
change in the mucosal integrity with resultant oesophagitis. Overflow
and aspiration are responsible for the respiratory symptoms associated
with this condition. The condition is associated with a late incidence of
oesophageal carcinoma. 3
History
Multiple, quite disparate presentations make achalasia a difficult diag-
nosis in some children. The diversity of symptomatology, ranging from
foregut symptoms to advanced pulmonary sepsis as a consequence of
aspiration, can distract from the diagnosis. The relative rarity of the
condition compounds the situation. Nevertheless, typical features are
pain on swallowing, dysphagia, vomiting, failure to thrive, and respira-
tory symptoms including chronic lung sepsis with wheezing. A family
history of achalasia is present on rare occasions.
Figure 50.1: Typical barium swallow in an oesophageal achalasia patient.