
Page 1 - 63 craniocerebral-and-spinal-trauma30-35_opt
P. 1
CHAPTER 30
Craniocerebral and Spinal Trauma
Bello B. Shehu
Mohammed R. Mahmud
Craniocerebral Trauma
Introduction
Paediatric cranial injuries constitute a major portion of paediatric admis-
sions and are the cause of the greatest number of deaths and chronic
disabilities among children. Brain injuries are responsible for 7,000 pae-
1
diatric deaths per year in the United States. The figures are quite a bit
higher in Africa, with various figures being quoted in different regions.
Paediatric cranial injuries are a challenge to manage, requiring difficult
decisions in a setting of limited resources. As in the developed coun-
tries, the socioeconomic impacts of head injury are enormous, including
school failure, social maladjustment, and public liability.
Epidemiology
Adult cranial injuries are primarily diseases of young men, with a male-
to-female ratio of 3–4:1. The sex ratio disparity is less in children; in all
age groups, including infants, the boy-to-girl ratio is about 2 to 1. The
2
great majority of cranial injuries in children are mild (86%). Severe
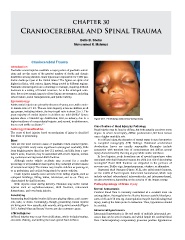
injuries show a bimodal age distribution; first, in infancy, due to a Figure 30.1: Penetrating orbitocranial foreign body.
higher incidence of nonaccidental injuries, and second, in adolescence,
due to road traffic accidents. 3–5
Classification of Head Injury by Pathology
Aetiology/Classification Head injuries may be focal or diffuse, but both actually coexist to some
The cause of head injuries based on mechanism of injury is classified degree. In severe head injury, diffuse predominates, but focal lesions
into blunt or penetrating. carry a higher mortality rate.
Blunt In a diffuse injury, the alteration of mental status is out of proportion
Falls are the most common cause of paediatric blunt cranial injuries. to computed tomography (CT) findings. Rotational acceleration/
Low-height falls rarely cause significant neurological morbidity. Falls deceleration forces are usually responsible. Examples include
from heights greater than four feet (1.2 meters), and falls from a care- concussion with transient loss of consciousness and diffuse axonal
taker’s arms, however, may be associated with severe injuries, includ- injury characterised by shearing at grey-white matter interfaces.
ing contusions and depressed skull fractures. In focal injuries, scalp lacerations are of special importance when
Although motor vehicle accidents may account for a smaller associated with skull fractures because the child is at risk of developing
6
percentage of all paediatric head injuries, they outweigh all other causes meningitis. Basal skull fractures are suspected in the presence of
of serious head injury. The trauma may involve children as passengers, raccoon eyes, Battles sign, haemotympanum, otorrhea, or rhinorrhea.
or as pedestrians and cyclists being struck by motor vehicles. Depressed skull fractures (Figure 30.2), also called pond fractures,
Crush injuries usually occur at home from falling objects, such as are the results of focal impacts. Intracranial haematomas, which may
collapsed buildings, falling tables, televisions, and so on. They are include epidural subarachnoid, intraventricular, and intraparenchymal,
characterised by skull fractures. are also prominent, depending on the severity of the impact energy.
Birth injuries occur during delivery. Neonates may suffer cranial Pathophysiology of Brain Injury
injuries such as cephalhaematomas, skull fractures, intracranial Normal homeostasis
haematomas, and even brain injuries.
Cerebral blood flow is normally maintained at a constant level via
Penetrating autoregulation. Autoregulation is effective between systolic blood pres-
Penetrating head injuries involve falls unto playing objects such as pen- sures of 50 and 150 mm Hg. Autoregulation may be lost following head
cils, nails, or sticks. Increasingly, though, penetrating cranial injuries injury, making the brain prone to ischaemia. Thus, hypotension should
are being seen from assaults, stab wounds, and gunshot wounds (Figure be avoided.
30.1). Animal bites and horses’ hooves are also common causes.
Intracranial hypertension
Inflicted injuries Intracranial hypertension is the end result of multiple intracranial pro-
Inflicted injuries may occur from child abuse, which includes beating, cesses that can be seen in trauma and which impair the cerebral blood
excessive shaking, and striking the head against hard surfaces. flow. Cardiorespiratory compensatory processes produce hypertension