
Page 8 - 61 surgical-infection&infestations20-24_opt
P. 8
Necrotising Fasciitis 131
Complications
Common complications that may be encountered include:
1. compartment syndrome, leading to Volkmann’s ischaemia,
Volkmann’s ischaemic contracture, or gangrene;
2. septic arthritis or osteomyelitis;
3. septicaemia and multiple organ failure syndrome;
4. herniation of intraabdominal organs;
5. joint stiffness; and
6. contractures and trismus.
Clinical Presentation
A high index of suspicion is required to ensure prompt recognition and
early treatment of NF. In the past, a significant number of affected chil-
dren died at home at the stage of inflammation as a result of toxaemia,
before getting to the hospital. With the advent of antibiotics, a signifi-
cant number of these children are now seen in hospitals (Figure 21.4).
Most studies report a slight male preponderance, but any age group can
be affected, including neonates and older children. In some studies, up
to 40% of these children have malnutrition. 8,13
The clinical presentation depends on the stage of NF at the time of
presentation (see Table 21.1). The commonly encountered symptoms
include pain, swelling, and fever. Although severe local pain that is out
of proportion to the size and type of wound is a hallmark of NF in older
children, this might be difficult to elucidate in neonates.
At the initial stages of cellulitis (inflammation), examination
will reveal features of toxaemia, including elevated temperature (or
hypothermia in neonates), oedema, hyperaemia, crepitus, tachycardia,
and hypotension. Blebs and blisters may precede the appearance
of dark skin patches (Figures 21.1, 21.4, and 21.5) that signify
tissue necrosis, usually with severe undermining. Late presentation is
common in Africa, and some patients are seen when the necrotic part
of the skin, subcutaneous tissues, and fascia come out together as a
complete cast from a limb (Figure 21.5). This exposes the underlying
muscle(s), tendon(s), or teeth and oral cavity in the case of the cheek.
Occasionally, some children are seen with structural deformities as a
result of improper management of the earlier stages of the disease.
The clinical presentation of Vibrio NF is similar to classical NF
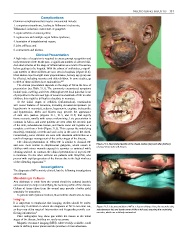
and even more similar to streptococcal gangrene, which occurs in Figure 21.4: Necrotising fasciitis of the cheek, before (top) and after (bottom)
removal of necrotic soft tissues.
children with minor wounds exposed to seawater or sustained while
cleaning seafood. In contrast, the clinical presentation of mycotic NF
is insidious. On the other extreme are patients with StrepTSS, who
present with rapid progression of the disease due to the high virulence
of the offending organisms. 23
Investigations
The diagnosis of NF is mainly clinical, but the following investigations
are relevant.
Microbiologic Cultures
Any discharge or swab from the wound should be cultured (aerobic
and anaerobic) to help in identifying the bacteria profile of the disease.
Culture of tissue taken from the wound may provide a better yield,
especially for anaerobes.
In patients with systemic features, blood culture should also be done.
Imaging
It is important to emphasize that imaging studies should be under-
taken only in children in whom the diagnosis of NF is not clear cut, Figure 21.5: Late presentation of NF in a 9-year-old boy. Here, the necrotic skin,
as they may delay surgical intervention and frequently provide con- subcutaneous fat, and fascia came off like a full cast, exposing the underlying
4
flicting information. muscles, which are relatively uninvolved.
Plain radiographs may show gas within the tissues at the initial
stages of the disease, but they are rarely necessary.
Magnetic resonance imaging (MRI), where readily available, could
assist in defining tissue planes and the presence of microabscesses.