
Page 14 - 61 surgical-infection&infestations20-24_opt
P. 14
Haematogenous Osteomyelitis and Septic Arthritis 137
the essential modality in the treatment of all stages of osteomyelitis in
LWATs.
Stage 1 HO is the most important stage for expeditious treatment,
which may result in cure of the acute process and also prevent
progression to chronic osteomyelitis. In acute HO, the operative goal
is to decompress all pus under pressure. This involves decompression
of both subperiosteal and intramedullary pus. Decompression must
be adequate enough to prevent reaccumulation. Antibiotics are highly
recommended in the initial treatment of stage 1 HO to manage the
systemic sepsis. Antibiotics are also recommended for a 2–6 week
period of treatment to prevent progression to chronic osteomyelitis.
Whenever HO has progressed to stage 2, x-ray changes already
indicate nonviable bone while systemic and local sepsis remains.
Treatment for stage 2 also involves prompt decompression and
antibiotics to treat the systemic sepsis. Usually, the sequestrum is not
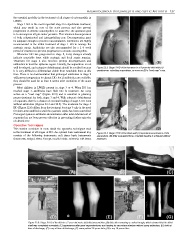
well developed, and extensive debridement should be avoided because Figure 22.3: Stage 3 HO of the humerus in a 5-year-old child with (A)
it is very difficult to differentiate viable from nonviable bone at this spontaneous extruding sequestrum, as seen on (B) a “road map” x-ray.
time. There is no documentation that prolonged antibiotics in stage 2
will prevent progression to chronic HO, but if antibiotics are available,
they should be used for at least 2 weeks after resolution of the acute
process.
Most children in LWATs present in stage 3 or 4. When HO has
reached stage 3, antibiotics have little role in treatment. An x-ray
serves as a “road map” (Figure 22.3) and is essential in planning
proper treatment for both stages 3 and 4. With adequate debridement
of sequestra, there is a chance of eventual healing of stage 3 HO even
without antibiotics (Figures 22.4 and 22.5). The treatment for stage 4
HO (Figure 22.6) differs from the treatment for stage 3 only in the need
for short-term antibiotics until the systemic sepsis has been controlled.
Prolonged systemic antibiotic administration after total debridement of
sequestra has not been proven effective in preventing further episodes
of chronic HO.
Operative Techniques
This section considers in more detail the operative techniques used
in the treatment of all stages of HO. An optimal basic instrument tray Figure 22.4: Stage 3 HO of the fibula with (A) spontaneous extrusion of the
consists of the following instruments: soft tissue basic instruments sequestrum. (B) After sequestrectomy, complete healing is achieved without
(haemostat, scalpel, tissue forceps, needle holder, scissors); soft tissue antibiotics.
Figure 22.5: Stage 3 HO of the tibia in a 7-year-old male: (A) initial presentation; (B) tibia after removing a cortical trough, which showed that the tibial
shaft was completely nonviable; (C) appearance after giant sequestrectomy and healing by secondary intention without using antibiotics; (D) child at
time of discharge; (E) x-ray at time of discharge; (F) same patient 15 years later; (G) x-ray 15 years later.